
KEYWORDS: Pulse oximeter; COVID-19; SARS CoV-2; hypoxia; hypoxemia; oxygen saturation; arterial blood gas analysis
INTRODUCTION:
In paroxysmal epidemic explosions, viral pneumonia has taken a heavy toll on humanity. Worldwide, COVID-19 (Corona Virus Infectious Disease 2019) causing SARS-CoV2 has killed millions of people. COVID-19 primarily affects the lungs. In severe cases, it leads to hypoxia and death. The pulse oximeter and arterial blood gas analysis aid the detection of hypoxia.1 Some shortcomings of these devices have been brought out in various studies in different contexts.2 One such study showcases a harrowing case series of three patients who showed ‘Happy hypoxia,’ where pulse oximeters failed to show the actual hypoxia.3 We assessed the utility of pulse oximeters in patients with SARS-CoV2 pneumonia.
METHODOLOGY
We recruited 48 COVID-19 pneumonia patients at the ICU of a tertiary Medical School and Hospital from July to December 2021. The sample size was calculated to detect a bias of at least 2% between SpO2(Oxygen saturation by pulse oximeter – Dr. Trust Series) and SaO2(Oxygen saturation by Arterial Blood Gas analyzer – ABL FLEX Radiometer Medical, Copenhagen, Denmark, installed in the ICU) with 80% power. The patients were diagnosed according to the WHO criteria.4 Patients with previous cardiorespiratory disorders were excluded. The pulse oximeter was applied to the finger, and blood for arterial blood gas analysis was taken simultaneously. The SpO2 value was compared against the SaO2 value from ABG analysis. Bland Altman analysis was used for direct comparison of quantitative values. The sensitivity and specificity of the pulse oximeter in detecting hypoxia [defined as SaO2 < 90% and defined as a PaO2 < 60 mm Hg] was calculated.5 Statistical analysis was performed with IBM SPSS Statistics for Windows, version 21 (IBM Corp., Armonk, NY, USA). Data is presented with a median and range. The p-value was calculated with the Mann-Whitney U test. Written informed consent was taken from the patients for the study.
RESULTS
Amongst the 40 patients who consented to participate in the study, the mean age of the subjects was 58.67±11.74 years, with 30.3% women. The mean SpO2 was higher (95±5.47) than the mean SaO2 (91.35±13.19). p=0.0383. 95% CI 0.2 to 7.10.
Bland Altman’s analysis revealed a bias of 1.77% and the limits of agreement -24.51% and 28.04% (Figure 1). On average, pulse oximetry (SpO2) shows about 1.77% more value than ABG(SaO2); it may show a reading as high as 28.04 above the ABG and as low as 24.51 than ABG at the extremes.
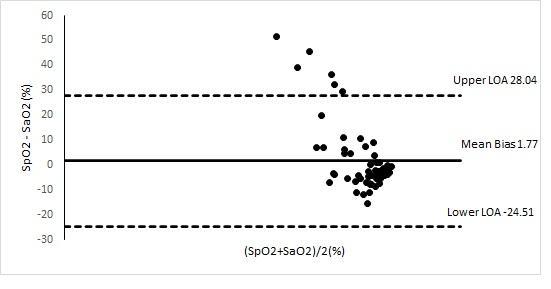
Figure 1: Bland Altman graph of SpO2 vs SaO2
In our study, ABG analysis (SaO2 < 90 measurement had 100% sensitivity and specificity in detecting PaO2 < 60 mm Hg). But pulse oximetry, with a sensitivity of only 50%, cannot detect hypoxia at a reading of SpO2 < 90%. At a SpO2 reading cutoff of 92, the sensitivity rose only to 65%. (Table 1) With a specificity of 76.09%, the ability of pulse oximeter reading of SpO2 < 90% to point out hypoxia was less. When the cutoff was taken at SpO2 < 92%, it presented an even higher proportion of 30.4% having hypoxia even when non-hypoxemic existed. The ROC curve, therefore, showed an AUC of 0.5, reiterating the pulse oximeter’s poor utility in detecting hypoxia in COVID-19 patients. The statistical correlation between SpO2 and SaO2 was poor (r=0.16).
Table 1: Sensitivity and Specificity of pulse oximeter
DISCUSSION
We studied pulse oximeter performance in 40 patients with COVID-19 pneumonia and found that pulse oximetry erred in detecting hypoxia. On average, the pulse oximeter showed a 1.77% higher value than SaO2. A previous study with children showed a bias of 3.3%,6 while older studies reported a bias of 1.7 to 2.5.7 This bias is dangerous. It would show patients with hypoxia as not having hypoxia. This may be one of the reasons for the happy hypoxia highlighted by the extensive use of pulse oximeters in the COVID-19 pandemic.
At both the cutoff SpO2 values of 90 and 92, pulse oximetry failed to detect hypoxia when there was hypoxia and also showed hypoxia when there was none. There was a poor correlation between SpO2 and SaO2 or PaO2 values. Similar results have been found in COVID-19 patients in a recent study.8
In COVID-19, arterial hypoxemia is thought to be induced by intrapulmonary shunting, dysregulated hypoxic pulmonary vasoconstriction, impaired lung diffusion, and formation of intravascular microthrombi. This causes tachypnea and hyperpnea. The consequent CO2 washout shifts the oxygen dissociation curve to the left. So, SpO2 is high even with suboptimal PaO2. The alveolar gas equation also shows a higher SpO2 recording in this type of pathology.3
The lung mechanics are well-preserved early in the disease, and there is no increased airway resistance or dead space ventilation. There is no CO2 build-up (the key driver for dyspnea), and the patients are aware of the hypoxia late. This happy hypoxemia is also noted in high altitude sickness.3
A recent study with COVID patients suggests that high ferritin and fibrinogen levels, which are acute phase reactants, may be associated with poor pulse oximetry performance.8 Other reasons for decreased pulse oximeter accuracy with hypoxemia include a paucity of reliable human calibration data during extreme hypoxia and an increased proportion of reduced hemoglobin in hypoxia, which can produce errors in the absorption ratio.9
An Australian study in 2020 showed that the ROC curve for SpO2 < 92% had 100% sensitivity and 84.4% specificity for detecting SaO2 < 90% and 95.1% sensitivity and 90.0% specificity for detecting PaO2 < 60 mmHg.5 However, our ROC data suggests minimal utility of SpO2 in detecting hypoxia. Therefore, the heterogeneity of the patients in the Australian study and their pathophysiologies may have contributed to the results.
There are limitations to this study. First, the single-center nature of the study decreases generalizability, and then the small sample size also reduces the power of the study.
CONCLUSION
Our study suggests that the pulse oximeter has significant limitations in assessing hypoxia in COVID-19 patients; hence, its role must be re-evaluated. This should be considered in the periodic severe viral pneumonia epidemics occurring worldwide.
CONFLICT OF INTERESTS STATEMENT
The authors declare no conflict of interest.
SOURCE OF FUNDING
None
AUTHORS’ CONTRIBUTIONS
SA: Conceptualization, Investigation, Methodology, Analysis, Supervision, Data curation, Writing the draft
KVRA: Investigation; Methodology; Analysis; Review and editing
SHB: Investigation; Methodology; Analysis; Review and editing
JPJ: Investigation; Methodology; Analysis; Review and editing
REFERENCES
1. Teo J. Early Detection of Silent Hypoxia in Covid-19 Pneumonia Using Smartphone Pulse Oximetry. J Med Syst. 2020;44(8):134.
2. Jubran A. Pulse oximetry. Crit Care. 2015;19(1):272.
3. Dhont S, Derom E, Van Braeckel E, Depuydt P, Lambrecht BN. The pathophysiology of ‘happy’ hypoxemia in COVID-19. Respir Res. 2020;21(1):198.
4. Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA. 2020;324(8):782-93.
5. Pilcher J, Ploen L, McKinstry S, et al. A multicentre prospective observational study comparing arterial blood gas values to those obtained by pulse oximeters used in adult patients attending Australian and New Zealand hospitals. BMC Pulm Med. 2020;20(1):7.
6. Ross PA, Newth CJ, Khemani RG. Accuracy of pulse oximetry in children. Pediatrics. 2014;133(1):22-9.
7. Van de Louw A, Cracco C, Cerf C, et al. Accuracy of pulse oximetry in the intensive care unit. Intensive Care Med. 2001;27(10):1606-13.
8. Gürün Kaya A, Öz M, Akdemir Kalkan İ, et al. Is pulse oximeter a reliable tool for non-critically ill patients with COVID-19?. Int J Clin Pract. 2021;75(12):e14983.
9. Wilson BJ, Cowan HJ, Lord JA, Zuege DJ, Zygun DA. The accuracy of pulse oximetry in emergency department patients with severe sepsis and septic shock: a retrospective cohort study. BMC Emerg Med. 2010;10