

KEYWORDS: Cytopenia, hyperferritinemia, lymphohistiocytosis, splenomegaly, typhoid fever
BACKGROUND
Hemophagocytic syndrome, or hemophagocytic lymphohistiocytosis (HLH), is an acute and rapidly progressive systemic hyper-inflammatory disorder characterised by cytopenia, excessive cytokine production, and hyperferritinemia. HLH consists of fever, splenomegaly, and cytopenia (at least affecting two cell lineages) due to hemophagocytosis in bone marrow, liver, or lymph nodes. It may be primary (familial) or secondary (acquired). Several bacterial, viral, fungal, and parasitic infections, autoimmune, malignant, and metabolic conditions can cause secondary HLH, which complicates the underlying disease progression and further increases the mortality of the underlying disease if required action is not taken early. Regardless of the aetiology, HLH in adults is associated with around a 50% mortality rate.1
Although several infectious agents have been implicated in causing HLH, enteric (or typhoid) fever has been documented only in a few cases.2 World Health Organization (WHO) estimates the global enteric fever disease burden at 11-20 million cases annually, resulting in about 128,000–161,000 deaths yearly.3 Uncommon complications of enteric fever whose incidences are reduced by prompt antibiotic treatment include disseminated intravascular coagulation, hemophagocytic syndrome, pancreatitis, hepatic and splenic abscesses and granulomas, endocarditis, pericarditis, myocarditis, orchitis, hepatitis, glomerulonephritis, pyelonephritis and hemolytic uremic syndrome, severe pneumonia, arthritis, osteomyelitis, endophthalmitis and parotitis.4 In developing countries like India, enteric fever is more common than in Western countries. Thus, findings consistent with HLH warrant an aggressive treatment approach and isolation measures to reduce the risk of superadded infection and mortality of the disease, especially in the context of developing countries like India, where healthcare facilities and the availability of appropriate antibiotics are a challenge.5
We present here two cases of HLH secondary to enteric fever, their treatment, and outcomes.
CASE PRESENTATION
Case One
A lady in her 30s, with no known prior comorbidity, presented to the Medicine OPD with complaints of acute, intermittent, high-grade fever for the last four days documented up to 1030F associated with chills and rigor. It was associated with dull aching, continuous, mild visceral type of abdominal pain along with nausea. There were no complaints of rash, cough, joint pain, vomiting or loose stool. Symptomatic medications were prescribed, and routine blood investigation (total cell count, liver function test and renal function test) along with tropical fever workup (TyphiDOT IgM, immunochromatography for malaria, scrub typhus, dengue NS1), blood culture and chest X-ray were advised.
After four days, the patient came back with reports and complaints of persistent symptoms along with newly developed symptoms of loose stool, 3-4 episodes a day.
On the 2nd visit, her heart rate was 104/min, her oxygen saturation was 94% on room air, her blood pressure was 86/56 mmHg, and she was tachypneic. Upon physical examination, the patient looked pale and dehydrated. There were no jaundice, oedema, lymphadenopathy or skin rashes. On systemic examination, the patient had a splenomegaly of 2 cm from the costal margin. The patient was admitted, intravenous (IV) access was secured, a blood sample was withdrawn, and resuscitation with IV fluid was started along with an empirical antibiotic ceftriaxone 2 gm 12 hourly, each infused over 4 hours.
The initial blood picture of the first OPD visit showed decreased leukocyte counts and reduced platelets (Table 1). Her repeat blood samples showed anaemia, leukopenia, and thrombocytopenia on admission. Peripheral smear showed normocytic normochromic red blood cells (RBC) with occasional nucleated cells, leukopenia with neutrophilic preponderance and markedly reduced platelet count. The reticulocyte count was 0.92% (corrected reticulocyte count 0.67%), and a prothrombin time (PT) of 10.4 seconds. Kidney function tests were normal. The liver function tests showed mild transaminitis.
Looking at her blood picture, sepsis was suspected. Ultrasound abdomen showed splenomegaly of size 17 cm. The inflammatory markers were elevated: ESR of 65 mm/hr, C-reactive protein (CRP) of 51 mg/L, and ferritin of 4000 ng/mL. Lactate dehydrogenase (LDH) was also high (358 U/L), including triglyceride of 210 mg/dL and fibrinogen of 205 g/L. Direct and indirect coomb tests were done to evaluate the drop in haemoglobin and cell count, which were negative.
There were no malarial parasites on peripheral blood smear. Viral serology for hepatitis viruses B, C, and E and human immunodeficiency virus (HIV), dengue virus non-structural protein 1 (NS1), and dengue IgM/IgG were negative. Typhi DOT IgM was positive; blood culture grew Salmonella Typhi susceptible to ampicillin, azithromycin, ceftriaxone, cefixime, chloramphenicol, and cotrimoxazole. H score was 234 points; 98-99% probability of HLH.6,7 HLH secondary to enteric fever was suspected. The patient did not consent to the bone marrow examination.
The patient was managed with intravenous ceftriaxone (2 gm IV BD for 7 days) followed by a tablet of azithromycin (1 gm OD for 5 days), and the patient improved both clinically and based on clinical parameters. The addition of azithromycin was due to clinical suspicion of failure to ceftriaxone on day 7, with persistent fever despite in vitro susceptibility. Cytopenia improved, and inflammatory markers also reduced with time.
Case Two
A man in his 40s, with a known history of type 2 diabetes mellitus for the last 9 years, presented to the emergency department with complaints of acute, intermittent, high-grade fever for the previous eight days documented up to 1040F associated with chills and rigor, which used to subside with oral medication, with no diurnal variation. It was associated with dull aching, continuous, mild visceral-type abdominal pain, with loose watery stool initially 4-5 episodes/day, without any episode of hematochezia or melena.
The initial physical examination at triage revealed a Glasgow Coma Scale (GCS) of 15/15, a respiratory rate of 28 breaths/min, a heart rate of 93/min, 96% oxygen saturation on room air, blood pressure of 90/60 mmHg and a normal axillary temperature. On physical examination, the patient looked markedly pale and dehydrated, for which intravenous access was secured, a blood sample was withdrawn, and intravenous fluid was started. He had a palpable spleen and liver. There were no signs of jaundice, oedema, visceromegaly, lymphadenopathy or skin rashes.
The initial blood picture showed pancytopenia (Table 2). Peripheral smear showed normocytic normochromic red blood cells (RBC) with occasional nucleated cells, leukopenia with neutrophilic preponderance, and markedly reduced platelet count. The reticulocyte count was 0.87% (corrected reticulocyte count 0.55 %), and the prothrombin time (PT) was 11.1 seconds. Kidney function tests showed prerenal acute kidney injury. The liver function tests showed moderate transaminitis. Ultrasound abdomen showed mild fatty liver with splenomegaly (16 cm).
Viral serology for hepatitis B, C, and E viruses, HIV, dengue virus non-structural protein 1 (NS1), and dengue IgM were negative. There were no malarial parasites on peripheral blood smear. Reticulocyte count showed a picture of hypo-proliferative marrow despite a normal serum total iron binding capacity level, serum folic acid and Vitamin B12. Direct and indirect Coomb’s tests were found to be negative. Blood culture grew Salmonella Typhi sensitive to azithromycin, chloramphenicol, and meropenem. Because of persistent pancytopenia, bone marrow aspiration and biopsy were done. The SGOT and SGPT values were raised.
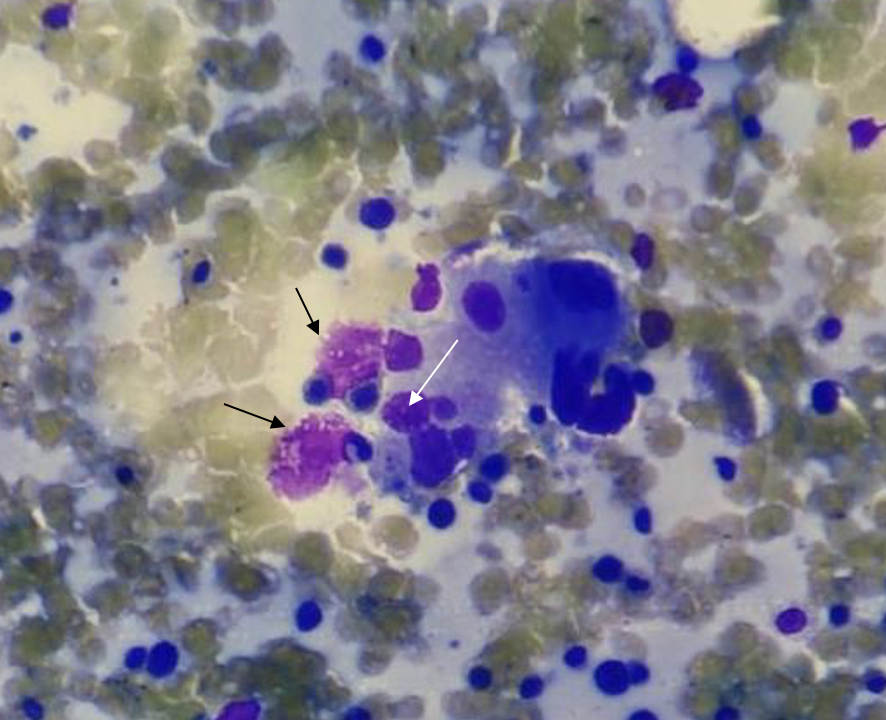
Further pertinent investigations were carried out to confirm HLH. Serum ferritin and triglycerides were quantified, and values were>10000 ng/ml and 294 mg/dL, respectively. Fibrinogen levels were low, with a value of 104 /L. Together with the clinical picture and laboratory data, these findings were compatible with a diagnosis of secondary HLH as per revised criteria of 2009 with an H score of 284 points; >99% probability of HLH.6,7 The patient was suspected to have HLH secondary to enteric fever and bone marrow aspiration, and a biopsy was performed with consent (Figure 1).
Figure 1. Bone marrow biopsy of case 2 showing leukopenia with normal distribution with no atypical cells, prominence of histiocytes (black arrow), and occasional evidence of hemophagocytosis (white arrow).
DISCUSSION
As already discussed, HLH is itself a rare entity. Still, it must be suspected in certain clinical and laboratory scenarios and must be treated aggressively once suspected, as the mortality rate is very high. Typical presenting signs and symptoms of HLH are nonspecific and usually related to organ damage by immune activation. Fever of unknown origin, cytopenia, splenomegaly, acute liver injury, bleeding, rash, and neurologic symptoms may all be indicative. Enteric fever is common in developing countries like India, Nepal, and other south Asian countries. With the availability of antibiotics and improving healthcare facilities, severe complications of enteric fever have been very rarely reported; still, in developing countries, HLH must be suspected and treated promptly following infections.3
The diagnosis of HLH is confirmed by fulfilment of one or both of the following criteria.8
1. A molecular diagnosis consistent with HLH
2. Five out of the following nine diagnostic criteria for HLH: fever, splenomegaly, cytopenias (affecting two or more of three lineages in the peripheral blood), hypertriglyceridemia (>265mg/dl) and/or hypofibrinogenemia (<150mg/dl), hyperferritinemia (>500mg/dl), hemophagocytosis in bone marrow/ spleen/ lymph nodes, low or absent natural killer (NK)-cell activity, elevated soluble CD25 (interleukin [IL]-2 receptor), elevated CXCL9.
Both of the cases presented in this report had a history of fever, splenomegaly and cytopenia involving all three lineages (red cell, leukocyte and platelet) and increased ferritin (1800 ng/ml in case1 and >1000 ng/mL in 2nd case). However, a bone marrow biopsy could not be done in the first case. Still, the patient had a very high H score. The bone marrow biopsy in the second case revealed the prominence of histiocytes with occasional evidence of hemophagocytosis. Based on the high H score of 234 points and 284 points, the diagnosis of HLH was made in both cases.
HLH can be primary, generally seen in children, and usually occurs due to genetic mutation.6 Secondary HLH, which occurs in adults, can be triggered by various causes including typhoid fever which may present as fever, diarrhoea and pancytopenia.9-11
The pathophysiology of secondary HLH is based on CD8+ T cells, which generate significant amounts of interferon-gamma (IFNγ), triggering the activation of macrophages. These overstimulated macrophages release inflammatory cytokines IL-1β, IL-6, IL-12, IL-18, and TNFα.Final_
In turn, the macrophage-produced IL-12 and IL-18 stimulate CD8+ T cells, intensifying the inflammatory response. The secondary tissue damage leads to the release of IL-33 and IL-1β, which further activates macrophages. Activated macrophages engulf blood cells and generate elevated levels of ferritin and pancytopenia. The resultant ‘cytokine storm’ underlies all clinical manifestations of HLH, ranging from endothelial damage to coagulopathy and multi-organ failure.12,13 The severity of organ damage may drastically deteriorate within hours, which warrants early suspicion, ICU admission and supportive management. Immunosuppression with a corticosteroid, intravenous immunoglobulins, and etoposide may be required based on the underlying aetiology and severity of organ dysfunction.14 Both patients were treated with antibiotics, resulting in an improvement in both symptoms and biochemical markers. In cases of critical organ involvement, chemotherapy with etoposide may be necessary, while intrathecal corticosteroids should be considered for central nervous system involvement.
CONCLUSIONS
Early suspicion and clear differentiation from sepsis are required to prevent worsening organ dysfunction, and treatment can be initiated before a definitive diagnosis of HLH. Although haematological malignancy like acute leukaemia presents as fever with pancytopenia, infective aetiology with secondary complications should be thought of in a country like India. The significance of early initiation of broad-spectrum empirical antibiotics should not be overlooked. This approach is essential to address potential bacterial infections promptly, given the overlapping clinical features between HLH and sepsis.
INFORMED CONSENT
Written informed consents were obtained from patients. The confidentiality of the patients was maintained in the article.
CONFLICTS OF INTEREST STATEMENT
The authors declare no conflict of interest.
SOURCE OF FUNDING
None
AUTHOR’S CONTRIBUTION
DD: Data collection; Analysis; Writing the draft
DK: Data collection; Analysis; Writing the draft
PKP: Conceptualization; Investigation; Methodology; Resources; Review & Editing
REFERENCES
Bichon A, Bourenne J, Allardet-Servent J, et al. High Mortality of HLH in ICU Regardless Etiology or Treatment. Front Med (Lausanne). 2021;8:735796.
WHO. Typhoid fever. World Health Organization. Accessed September 28, 2024. https://www.emro.who.int/health-topics/typhoid-fever/
Meazza Prina M, Martini F, Bracchi F, et al. Hemophagocytic syndrome secondary to SARS-Cov-2 infection: a case report. BMC Infect Dis. 2021;21(1):811.
Pandey M, Dhingra B, Sharma S, Chandra J, Pemde H, Singh V. Enteric Fever presenting as secondary hemophagocytic lymphohistiocytosis. Indian J Pediatr. 2012;79(12):1671-2.
Sánchez-Moreno P, Olbrich P, Falcón-Neyra L, Lucena JM, Aznar J, Neth O. Typhoid fever causing haemophagocytic lymphohistiocytosis in a non-endemic country – first case report and review of the current literature. Enferm Infecc Microbiol Clin (Engl Ed). 2019;37(2):112-6.
Fardet L, Galicier L, Lambotte O, et al. Development and validation of the HScore, a score for the diagnosis of reactive hemophagocytic syndrome. Arthritis Rheumatol. 2014;66(9):2613-20.
Debaugnies F, Mahadeb B, Ferster A, et al. Performances of the H-Score for Diagnosis of Hemophagocytic Lymphohistiocytosis in Adult and Pediatric Patients. Am J Clin Pathol. 2016;145(6):862-70.
Hines M, Bhatt N, Talano JAM. Diagnosis, Treatment, and Management of Hemophagocytic Lymphohistiocytosis in the Critical Care Unit. Critical Care of the Pediatric Immunocompromised Hematology/Oncology Patient. 2018;159-82.
Abbas A, Raza M, Majid A, Khalid Y, Bin Waqar SH. Infection-associated Hemophagocytic Lymphohistiocytosis: An Unusual Clinical Masquerader. Cureus. 2018;10(4):e2472.
Non LR, Patel R, Esmaeeli A, Despotovic V. Typhoid Fever Complicated by Hemophagocytic Lymphohistiocytosis and Rhabdomyolysis. Am J Trop Med Hyg. 2015;93(5):1068-9.
George N, Sethi P, Nischal N, Kumar A, Siripurapu G, Wig N, Vyas S. A catastrophic presentation of enteric fever with secondary hemophagocytic lymphohistiocytosis. J Assoc Physicians India. 2018;66:11-2.
Benevenuta C, Mussinatto I, Orsi C, Timeus FS. Secondary hemophagocytic lymphohistiocytosis in children (Review). Exp Ther Med. 2023;26(3):423.
La Rosée P, Horne A, Hines M, et al. Recommendations for the management of hemophagocytic lymphohistiocytosis in adults. Blood. 2019;133(23):2465-77.
George MR. Hemophagocytic lymphohistiocytosis: review of etiologies and management. J Blood Med. 2014;5:69-86.