

KEYWORDS: Alcoholism; brain abscess; diabetes mellitus; secondary infection; septic emboli
INTRODUCTION
Diabetes mellitus and alcoholism are two of the most common conditions plaguing society today, causing a wide variety of health-related issues. Both cause immune dysregulation by a wide variety of mechanisms and predispose to complicated infections with a complicated hospital course, requiring higher antibiotics, increasing the cost of healthcare and morbidity. As compared to non-diabetics, people with diabetes were found to be 4.4 times more likely to develop sepsis of unknown origin.1 Similarly, alcoholics have more infections than non-alcoholics, in particular pneumonia and bacteremia.2
Bacteraemia, by definition, is the presence of bacteria in the blood and can be asymptomatic to metastatic severe infection. Metastatic or disseminated infection is a deep, distal, or secondary infection, anatomically unrelated to the primary site infection.3 Staphylococcus aureus bacteremia is the most common cause of metastatic infection. The risk of metastatic infection is increased by host factors such as smoking, alcoholism, old age, diabetes, and immunosuppression.4
We want to report this fascinating, unusual case with metastatic infection of unknown origin.
CASE PRESENTATION
The patient is a 44-year-old man with no known prior comorbidities and a history of chronic alcohol consumption for 20 years and chronic bidi consumption for 20 years, who was brought to the emergency department with a history of two episodes of focal seizures, 30 minutes apart, in the form of deviation of angle of mouth to the left and up rolling of eyes, followed by altered mental sensorium in the form of decreased responsiveness and loss of consciousness. There was no history of fever, headache, any history suggestive of tonic/clonic movements, no history of trauma, palpitations, cough, melaena, jaundice, or vomiting. There was no history of similar complaints in the past. There is no family history of seizures.On initial
assessment in the emergency department, the patient’s Glasgow Coma Score (GCS) was E1V1M3; the patient had poor oral hygiene with tobacco stains and dental caries. Bilateral pupils were reactive to light, and meningeal signs were absent. Serum electrolytes and blood sugar were within normal limits. Given low GCS, the patient was intubated and placed on mechanical ventilation in the emergency department. As his sensorium improved, he was extubated and liberated from mechanical ventilation. He was then admitted to the Department of Medicine for further evaluation.
Routines revealed elevated total leucocyte count (35.48 x 103 cells/cumm; Range: 4 – 11 x 103 cells/cumm) and elevated inflammatory markers [C-reactive protein = 200.6 mg/L (Range: 0 – 1 mg/L), erythrocyte sedimentation rate = 40 mm/hr]. Procalcitonin was elevated (4.11 ng/mL; Range: 0 – 0.5 ng/mL). Prothrombin time (PT)/international normalized ratio (INR) was 13.3/1.24, and platelet count was 144 x 103/uL (Range 150 – 450 x 103/uL). The NCCT head showed an ill-defined heterodense area with surrounding vasogenic edema in the right frontal lobe, causing a mass effect. The patient was subjected to a contrast-enhanced – MRI Brain, which revealed two peripherally enhancing lesions in the right frontal lobe, showing a lipid lactate peak on MR spectroscopy suggestive of brain abscess (Fig 1A-B-C).
Figure 1. Radiological images of the patient during hospital admission: Contrast-Enhanced – MRI Brain (A, B & C) showing peripherally enhancing lesion (arrows) with central T2 hyperintense area showing diffusion restriction with low values on ADC maps, seen in the right frontal lobe, larger measuring ~7.5x9mm suggestive of brain abscess; Contrast Enhanced – Computed Tomography – Thorax (D & E) showing multiple patchy areas of peripheral consolidation with surrounding ground glass opacities (arrows), some of them are showing feeding vessel in basal segments of bilateral lungs, largest measuring ~1.0×0.8 cm is seen in posterior basal segment of right lower lobe suggestive of septic emboli.
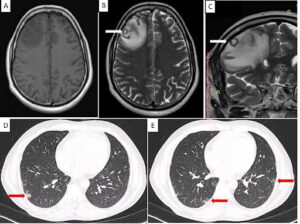
There was also adjacent leptomeningeal and pachymeningeal enhancement. CSF analysis showed mild pleocytosis (total count = 15 cells/cumm; 100% monomorphs); CSF sugar and protein were within normal limits (sugar = 81 mg/dL; Protein = 51 mg/dL). CSF culture, potassium hydroxide mount, India ink mount examinations and Cartridge based nucleic acid amplification test (CBNAAT) were all negative. Blood and urine cultures were sterile. Nasal scrapings were positive for Klebsiella pneumoniae. Fungal culture yielded no growth.
A diagnosis of multiple brain abscesses with meningitis was made, and the patient was started on empirical antibiotic therapy (meropenem 1gm IV 8 hourly and vancomycin 1gm IV 12 hourly) as per the latest guideline. The patient was also worked up to look for the source of the brain abscesses. A chest X-ray was suggestive of a cavitary lesion in the left lung field, and hence, CECT thorax was undertaken. It revealed multiple septic emboli (Fig 1D-E). Suspecting infective endocarditis, 2D echocardiography was done, which did not reveal any vegetation.
The patient was managed with parenteral antibiotics for six weeks, along with antiepileptics. He was started on insulin for diabetes and thyroxine supplementation for hypothyroidism. He was discharged on outpatient parenteral antibiotic therapy (same meropenem and vancomycin) with stable vitals. Repeat imaging was undertaken at monthly intervals. The first scan, done one month post-treatment, revealed resolving abscesses, and the subsequent scan at two months showed no residual abscess with gliosis. The patient was counseled regarding alcohol abstinence, which he followed judiciously. He resumed all daily activities within a few weeks of being discharged.
DISCUSSION
This case represents metastatic infection in the brain and lungs in immunosuppressed states due to diabetes and alcoholism, but the primary source couldn’t be identified. In only about 41 % of metastatic infections, signs and symptoms of primary source could be identified or treated.5 Hence, the primary focus of metastatic infection can be unknown, similar to sepsis of unknown origin.
Diabetes mellitus and chronic alcoholism compromise the immune function of the body by various mechanisms. Immune dysfunction in diabetes is proposed to be occurring via the following mechanisms: impaired cytokine production, impaired recruitment of leukocytes, defective pathogen recognition due to downregulation of toll-like receptors (TLRs), neutrophil dysfunction, macrophage dysfunction, natural killer (NK) Cell dysfunction, antibody and complement effector inhibition.6
Chronic alcoholism also causes immune dysfunction.7 The gut is usually the first part that comes into contact with alcohol. Here, it disrupts mucosal integrity, thus facilitating the translocation of microorganisms into the systemic circulation. Alcohol consumption also alters the gut microbiota, which is essential for the maturation and function of the immune system. The resulting gut dysbiosis impairs this interaction between the microorganisms and the immune system. In the respiratory tract, alcohol impairs ciliary function in the upper respiratory tract and impairs the function of alveolar macrophages and neutrophils, that is, the respiratory cells of the immune system. In studies, it has also been shown that acute binge alcohol consumption and not just chronic alcohol consumption affects the immune system.
Metastatic infections are quite commonplace in diabetic patients yet appear to be underreported. Bader et al reported 12 patients with diabetic foot infection with distant metastatic foci of infection, including endocarditis, septic arthritis, and spine infections, of whom three passed away, and three had a recurrence of infection.8 The organism identified was S. aureus. Shaho et al reported another case of metastatic spinal abscesses from diabetic foot osteomyelitis – the patient was managed aggressively, but developed significant morbidity in the form of severe paraparesis.9 Tsai et al reported a case of metastatic endophthalmitis with a subretinal abscess in a 56-year-old patient with uncontrolled diabetes.10 The primary source was a liver abscess. In another case reported by Katsuura et al, the primary source of a metastatic S. aureus infection of the spine and extremities in a diabetic patient could not be identified.11
In the present case, who happened to have predisposing risk factors of chronic alcohol use and diabetes mellitus, we saw a disseminated infection without a known primary focus, which led to a complicated hospital course involving mechanical ventilation and a protracted course of higher antibiotics. The patient was thoroughly worked up and treated empirically with a course of meropenem and vancomycin for six weeks. He was later found to have Klebsiella pneumoniae. Prior studies also showed that K. pneumoniae infections are more frequent amongst people with diabetes as compared to non-diabetics.1 Our patient responded to therapy, and on serial imaging on subsequent follow-up visits, there was evidence of resolution of the cerebral metastatic infection. The patient also maintained strict glycaemic control and abstinence from alcohol, which also likely contributed to his recovery.
This case highlights the abstinence of chronic alcohol use and control of diabetes on patient outcomes. It also highlights the need for a high degree of clinical suspicion for disseminated infections in patients with diabetes, and the treating physicians should seek out other foci.
CONCLUSION
Diabetes mellitus and chronic alcoholism increase the risk for metastatic infections, which can have a varied presentation. Disseminated or secondary or metastatic infection can present with brain abscesses and septic lung emboli. Metastatic infection can present without primary focus.
INFORMED CONSENT
The patient provided consent to publish the case report. Confidentiality of the patient was maintained in the article.
CONFLICT OF INTERESTS STATEMENT
The authors declare no conflict of interest.
SOURCE OF FUNDING
None
AUTHORS’ CONTRIBUTIONS
BR: Data collection; Analysis; Writing the draft
SK: Data collection; Analysis; Writing the draft
PKP: Conceptualization; Investigation; Methodology; Resources; Critically review
RK: Supervision, Validation, Review & editing
REFERENCES
National Centre for Disease Control (NCDC). National AMR Surveillance Network (NARS-Net) Annual Report 2023. Accessed March 24, 2024. https://ncdc.gov.in/showfile.php?lid=1004
National Centre for Disease Control (NCDC). Surveillance of Antimicrobial Consumption under National Antimicrobial Consumption Network (NAC-NET) 2023. Accessed March 24, 2024. https://ncdc.gov.in/WriteReadData/l892s/7810983521691140244.pdf
Ministry of Health and Family Welfare (MoHFW). Government of India. Use of Antibiotics. Accessed March 24, 2024. https://pib.gov.in/PressReleaseIframePage.aspx?PRID=1524806
Stoeckle M, Kaech C, Trampuz A, Zimmerli W. The role of diabetes mellitus in patients with bloodstream infections. Swiss Med Wkly. 2008;138(35-36):512-9.
Sternbach GL. Infections in alcoholic patients. Emerg Med Clin North Am. 1990;8(4):793-803.
Horino T, Hori S. Metastatic infection during Staphylococcus aureus bacteremia. J Infect Chemother. 2020;26(2):162-9.
Ellis S, Ong E. Disseminated Infections: A Clinical Overview. Molecular Medical Microbiology. 2015;637-53.
Vos FJ, Kullberg BJ, Sturm PD, et al. Metastatic infectious disease and clinical outcome in Staphylococcus aureus and Streptococcus species bacteremia. Medicine (Baltimore). 2012;91(2):86-94.
Berbudi A, Rahmadika N, Tjahjadi AI, Ruslami R. Type 2 Diabetes and its Impact on the Immune System. Curr Diabetes Rev. 2020;16(5):442-9.
Sarkar D, Jung MK, Wang HJ. Alcohol and the Immune System. Alcohol Res. 2015;37(2):153-5.
Bader MS, Hawboldt J, Vincent Y, et al. Distant metastatic foci of infection in adult patients with diabetic foot – not as rare as we think?: case series and review of the literature. Infect Dis (Lond). 2021;53(4):255-73.
Shaho S, Khan S, Huda MS, Chowdhury TA. Metastatic spinal abscesses from diabetic foot osteomyelitis. BMJ Case Rep. 2014;2014:bcr2014204816.
Tsai TH, Peng KL. Metastatic endophthalmitis combined with subretinal abscess in a patient with diabetes mellitus–a case report. BMC Ophthalmol. 2015;15:105.
Katsuura Y, Cincere B, Cason G, Osborn J. Metastatic MSSA infection of the spine and extremities. BMJ Case Rep. 2018;2018:bcr2017222778.
Central Drugs Standard Control Organization (CDSCO). Rational Use of Antibiotics for Limiting Antimicrobial Resistance. Accessed March 24, 2024. https://cdsco.gov.in/opencms/resources/UploadCDSCOWeb/2018/UploadCircularFile/AMRMiscircular.pdf
Reed EE, Stevenson KB, West JE, Bauer KA, Goff DA. Impact of formulary restriction with prior authorization by an antimicrobial stewardship program. Virulence. 2013;4(2):158-62.