

KEYWORDS: Brucella, Intravenous immunoglobulins, Immune thrombocytopenia, Zoonosis
INTRODUCTION
Brucellosis is caused by Gram-negative coccobacilli belonging to Brucella spp. It is an infectious disease known by many names, such as remitting fever and Mediterranean fever. These bacteria are primarily zoonotic in origin and commonly found in various farm and wild animals’ reproductive organs and reticuloendothelial systems. The disease can be transmitted to humans through unpasteurized dairy, undercooked meat, or direct contact with infected animals and, hence, is common in people involved in livestock farming. Manifestations are often nonspecific, such as undulating fevers, generalized malaise, arthralgias, hepatosplenomegaly and skin rashes.1
Thrombocytopenia, a rare complication of brucellosis, occurs in 3% to 26% of cases.2-4 It involves low platelet counts, potentially causing spontaneous bleeding below 20,000/mL. Diagnosis requires a high index of suspicion in the setting of active Brucella infection. It includes a thorough history and series of laboratory investigations to exclude causes of low platelet counts. The exact pathogenesis behind this finding is unclear, but many possible mechanisms have been put forward. However, secondary immune thrombocytopenia is rare and has been infrequently and inconsistently reported in a few case reports.
CASE HISTORY
A 31-year-old male presented to trauma and emergency with a history of bleeding from gums for the last one-month, black tarry stools for one-month, petechial skin rashes for 12 days, and epistaxis for the previous two days. The patient was initially being managed at a local district hospital for 15 days, where he received multiple transfusions of Random Donor Plasma and Red cell concentrate, but ultimately referred to our institution due to non-resolution of symptoms. At the time of presentation to our institute, the patient had the above-given complaints and had no history of fever, cough, chest pain, abdomen pain, jaundice, or joint pain. The patient was a daily wage laborer at a construction site and had a social history of occasional alcohol consumption and smoking cigarettes. At presentation, the patient was vitally stable and afebrile.
On general examination, pallor was noticed. However, there were no signs of icterus, clubbing, cyanosis, lymphadenopathy, or oedema. Cardiovascular, respiratory, and neurological examinations were within normal limits; however, moderate splenomegaly was noted on abdominal examination.
On the patient’s initial workup, the complete blood count showed bi-cytopenia with a decrease in RBCs and platelets. Ultrasound of the whole abdomen showed hepato-splenomegaly. Hepato-splenic-portal doppler was done, and it showed a normal study with moderate splenomegaly. The patient was suspected to have ITP and started on pulse methylprednisolone 1gm/day for three days, followed by prednisone 60mg/day. Despite the intervention, a limited response in platelet counts was observed. On day 5 of admission, intravenous immunoglobulin (IVIG) was added to the treatment regimen at a dose of 1 gm/kg/day or five days, but no response was observed.
Further workup was done to ascertain the etiology of the thrombocytopenia. Dengue and malaria investigations returned negative. Peripheral smear showed microcytic hypochromic anaemia and thrombocytopenia. The iron profile showed iron deficiency anaemia (hemoglobin – 6g/dL, mean corpuscular volume – 72 fL, total iron binding capacity – 600 ug/dL, serum iron – 23 ug/dL, ferritin – 7 ng/dL). The source of this iron deficiency was suspected to be prolonged bleeding over the last one month. A hemophagocytic lymphohistiocytosis (HLH) workup was done but the laboratory investigation results did not fulfill the criteria for HLH. Bone marrow biopsy revealed a normocellular marrow and increased megakaryocytes. A contrast-enhanced computed tomography of abdomen and pelvis was done to rule out lymphoma and found to be normal. Romiplostim was started based on a Haematology consultation on day 5 of admission.
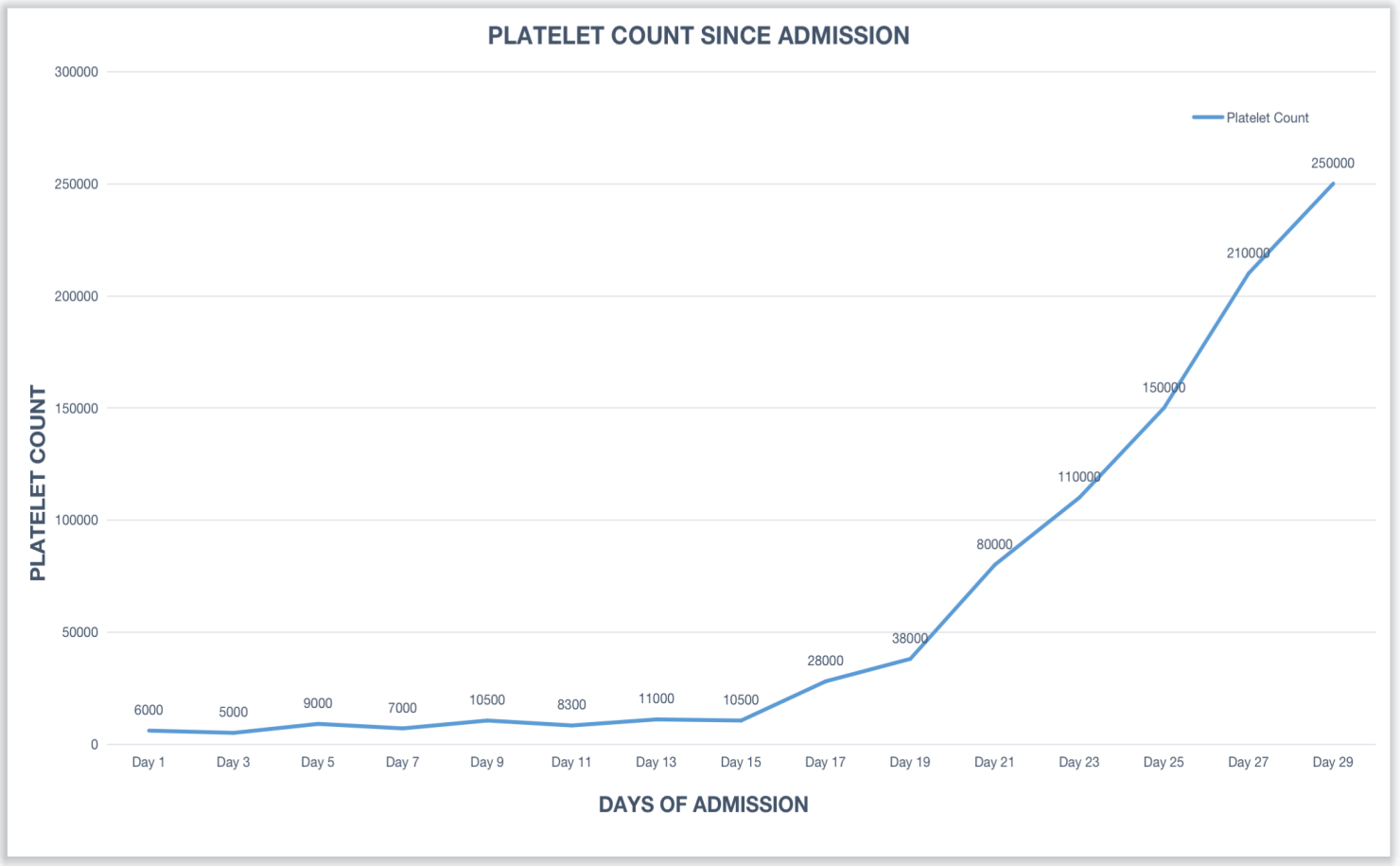
Infectious Disease consultation was sought, and investigations were sent for Venereal Disease Research Laboratory (VDRL) test for syphilis, Epstein-Barr Virus serology, Brucella serology, and RK-39 for leishmaniasis. Brucella IgM by the Enzyme-Linked Immunosorbent Assay (ELISA) tested positive on day 14 of admission. After joint consultation of hematology and infectious diseases experts, steroids were stopped, and the patient was started on oral doxycycline 100mg BD and intravenous gentamicin 350mg OD. Following one week of this therapy, the patient’s cell counts started to improve, and the platelet counts improved to 80,000/uL and further continued to improve [Figure 1].
Figure 1: Platelet count trend during hospitalization (diagnosis of Brucellosis was made and its management was started on day 14 of admission).
DISCUSSION
The case is a young male who presents with symptoms of bleeding and moderate splenomegaly on examination. Based on the preliminary evaluation, the patient is suspected to have primary idiopathic ITP managed with steroids and IVIG, but no clinical response is observed. On investigating secondary causes of ITP, the patient was found to have a positive IgM for Brucella, which was managed with oral and IV antibiotics and recovered.
Brucella is an important zoonotic pathogen that is often underdiagnosed in India due to indolent and waxing and waning symptoms and lower awareness among livestock herders. The organism prefers lymphoreticular and reproductive systems, thriving intracellularly to evade immune responses and antibiotics. Following its highly variable incubation period (ranging from days to weeks), the bacterium is transported via the intestinal submucosal lymphatics into the systematic lymphoreticular system, where it hides intracellularly, multiplies in various tissues, and gives rise to its pathological manifestations. They employ strategies like hindering vacuole-lysosome fusion, preventing cell apoptosis, and inhibiting dendritic cell function, aiding their persistence and pathogenicity.5
The most common symptoms associated with brucella infection are fever, rash, weakness, fatigue, night sweats, and arthralgias, which are highly nonspecific and contribute to its underdiagnosis.1 The infection manifests as various arthralgias, including sacroiliitis, osteomyelitis, spondylodiscitis, septic arthritis, and epidural abscess.6 It can also cause hepatic abscesses, granulomas, and spontaneous bacterial peritonitis. Respiratory symptoms like cough, dyspnea, and pleurisy may occur, with chest radiography often showing normal findings but sometimes revealing focal abscesses, effusions, or granulomas. Neurological symptoms such as Guillain-Barre syndrome, subarachnoid hemorrhage, and myelitis have also been associated with acute neurobrucellosis.7
Thrombocytopenia is a rare complication associated with brucellosis found in 3% to 26% of patients.2-4 Most of the cases described have been in the form of case reports.3,4,8-10 A milder decrease may only be a lab finding, whereas more severe thrombocytopenia (platelet counts <20000/uL) present as a purpuric rash, bleeding gums, epistaxis, gastro-intestinal bleeds and even intracranial hemorrhages which can be quickly fatal. The precise pathological characteristics of this process are unclear. However, some possible mechanisms have been proposed, including bone marrow suppression, hypersplenism, hemophagocytosis, and disseminated intravascular coagulation.4 However, immune-mediated destruction of platelets has been described in very few case reports. Possible molecular mimicry is implicated in this manifestation, leading to the autoimmune destruction of platelets. We suspected a similar mechanism of immune mediated thrombocytopenia secondary to molecular mimicry that led to catastrophic decrease in platelet count in our patient.
To treat uncomplicated brucellosis, a doxycycline-aminoglycoside combination is the first choice. Other oral regimens may be considered alternatives, including quinolones (e.g., ciprofloxacin or ofloxacin). Triple therapy should be used only in severe, complicated cases. For the prevention of multidrug-resistant tuberculosis, the prescription of rifampin in the treatment of brucellosis in TB prevalence areas should be limited.11
Thrombocyte recovery usually occurs within 1–3 weeks of initiating appropriate antimicrobial therapy. However, in cases of severe thrombocytopenia, an urgent glucocorticoid treatment will increase platelet count and can control bleeding until the antimicrobial therapy takes effect. If a patient has mild-to-moderate thrombocytopenia with no life-threatening bleeding, anti-brucellosis treatment should be started only. It is suggested that corticosteroids should be started along with anti-brucellosis therapy in cases where platelet count is < 10,000 per microlitre.12
CONCLUSIONS
It is crucial to have a high index of clinical suspicion for brucellosis as a potential cause when encountering isolated thrombocytopenia in areas where the disease is highly endemic. An alarm should especially be raised if a patient with a history of livestock farming has been increasingly experiencing persistent undulating fevers, myalgias, and arthralgias. While an uncommon cause, with an accurate diagnosis, treatment often leads to a remarkable recovery.
INFORMED CONSENT
Written informed consent was obtained from the patient. Confidentiality of the patient was maintained in the article.
CONFLICTS OF INTEREST STATEMENT
The authors declare no conflict of interest.
SOURCE OF FUNDING
None
AUTHOR’S CONTRIBUTION
SV: Investigation; Writing the draft
PB: Supervision; Investigation; Review & Editing
JS: Conceptualization; Validation; Review & Editing
REFERENCES
Bosilkovski M, Krteva L, Dimzova M, Vidinic I, Sopova Z, Spasovska K. Human brucellosis in Macedonia – 10 years of clinical experience in endemic region. Croat Med J. 2010;51(4):327-36.
Franco MP, Mulder M, Gilman RH, Smits HL. Human brucellosis. Lancet Infect Dis. 2007;7(12):775-86.
Young EJ, Tarry A, Genta RM, Ayden N, Gotuzzo E. Thrombocytopenic purpura associated with brucellosis: report of 2 cases and literature review. Clin Infect Dis. 2000;31(4):904-9.
Abdallah TM, Elbagi OMA, Karoum AO, Ali AAA. Acute brucellosis as unusual cause of immune thrombocytopenia: a case report and review of the literature. Asian Pac J Trop Biomed. 2014;4: 751–4.
de Figueiredo P, Ficht TA, Rice-Ficht A, Rossetti CA, Adams LG. Pathogenesis and immunobiology of brucellosis: review of Brucella-host interactions. Am J Pathol. 2015;185(6):1505-17.
Arkun R, Mete BD. Musculoskeletal brucellosis. Semin Musculoskelet Radiol. 2011;15(5):470-9.
Naderi H, Sheybani F, Parsa A, Haddad M, Khoroushi F. Neurobrucellosis: report of 54 cases. Trop Med Health. 2022;50(1):77.
Kamali Aghdam M, Davari K, Eftekhari K. Recurrent Epistaxis and Bleeding as the Initial Manifestation of Brucellosis. Acta Med Iran. 2016;54(3):218-9.
Rad ZA, Sajedi B, Akbarieh S, Heydari AH, Ali SB, Mojdehi AM. A case report of isolated thrombocytopenia induced by brucellosis. Asian Pac J Trop Dis. 2017; 7: 181–2.
Erkurt MA, Sari I, Gül HC, Coskun O, Eyigün CP, Beyan C. The first documented case of brucellosis manifested with pancytopenia and capillary leak syndrome. Intern Med. 2008;47(9):863-865.
Alavi SM, Alavi L. Treatment of brucellosis: a systematic review of studies in recent twenty years. Caspian J Intern Med. 2013;4(2):636-41.
Aon M, Al-Enezi T. Acute Brucellosis Presenting with Bleeding Tendency due to Isolated Severe Thrombocytopenia. Case Rep Infect Dis. 2018;2018:7867435.