

KEYWORDS: cefazolin; surrogate marker; cefixime; uncomplicated; urinary tract; infections
INTRODUCTION:
For uncomplicated urinary tract infections (uUTIs) caused by Escherichia coli, Klebsiella pneumoniae, and Proteus mirabilis, the increasing resistance patterns observed to oral antibiotics i.e. trimethoprim-sulfamethoxazole and fluoroquinolones has prompted oral third-generation cephalosporins (3GCs), namely cefpodoxime, cefdinir and cefixime, as viable alternative treatment options.1 Thus, timely reporting of oral 3GC susceptibility may avoid usage of other broad-spectrum antibiotics or intravenous therapy. However, many oral cephalosporin agents are unavailable for testing in automated susceptibility systems, and breakpoints for some oral cephalosporins still need to be elucidated. Surrogate testing allows clinicians to use the preferred oral cephalosporin without requiring the clinical laboratory to perform additional susceptibility testing separately.2
For E.coli, K. pneumoniae, and P. mirabilis isolates from uUTIs, CLSI (Clinical and Laboratory Standards Institute) recommends using cefazolin as a surrogate marker to predict susceptibility to seven oral cephalosporins, including the 3GCs cefpodoxime and cefdinir; however, it does not provide guidance for cefixime.3 Our aim was to determine whether cefazolin’s susceptibility results can predict susceptibility to cefixime amongst urinary isolates of E. coli, K. pneumoniae, and P. mirabilis isolated from cases of uUTIs.
HOW DID WE SRTART?
We started with the lowest-hanging fruit, our surgical prophylaxis (SP) practices.1 When we started, the antibiotics intended to be given as SP were continued for almost seven days and often continued at discharge. Broad-spectrum antibiotics were frequently given as SP. Realizing the need for a change, we reviewed the literature on surgical prophylaxis, collected the initial baseline data, and engaged with our surgical colleagues to build a consensus. Brainstorming sessions were held with surgeons, and evidence-based consensus was agreed upon and implemented. Our head of the Anaesthesia department was entrusted with the responsibility for this initiative. To begin with, monthly focussed audits were initiated for SP practices in 3 surgical specialties: coronary artery bypass grafting (CABG), total knee replacement (TKR), and laparoscopic cholecystectomy. Type, time of administration before surgical incision, and the duration of antibiotic(s) were looked explicitly into for compliance. A special note was also made regarding antibiotics prescribed at discharge. Compliance with these metrics was shared with respective shareholders and the medical administration at periodic intervals.
Many challenges were faced during the implementation phase, requiring multiple meetings with various specialties to address the concerns. In some specialties like CABG, it was the choice of antimicrobials; in others, it was the duration. It also required the simultaneous involvement of infection control, engineering, and central sterile supply department (CSSD) teams with the surgical teams to generate confidence in the operating room practices to reduce the fallback on antimicrobials as a risk reduction strategy. In certain specialties, a trade-off was also worked out between the clinical and administrative teams where the administration agreed to a particular brand of narrow-spectrum original antimicrobial in exchange for a reduced duration of the SP. Gradually, significant gains have been seen in our SP practices over the last few years, and the scope of surveillance now includes the following ten surgical specialties: CABG, TKR, craniotomy, laparoscopic cholecystectomy, hernia repair, cesarean section, spine surgery, renal transplant, vascular surgery – Arterio-venous (AV) fistula, and pediatric cardio-thoracic vascular surgery.
The core team addressed the medical antimicrobial prescriptions after finding success and streamlining the surgical prophylaxis. This was a significant challenge as our tertiary care center has to deal with referred and complicated cases from other hospitals with exposure to most classes of antimicrobials. The hospital has open intensive care units (almost 60% of the total bed strength of the hospital) with consultant-based practice – both employed and empaneled. This form of engagement had its challenges and advantages.
To define our areas of intervention, we needed to study our antimicrobial prescription patterns. Point Prevalence Surveys were conducted based on a defined tool, which captured various aspects of the antimicrobial prescription, including reasons for starting antimicrobials, combinations, number, duration, culture before starting antimicrobials, periodic review with labs, de-escalation, etc. A written document expressing the vision of our program, requirements, and measurables was created and shared with the management to request the necessary resources. A Lead Pharmacist with a keen interest in this field was appointed as a critical resource. A senior clinician intensivist with good standing and rapport with the medical fraternity was chosen as the champion for this initiative.
The first task was to expand the scope of our antimicrobial policy beyond surgical prophylaxis to include guidance on the empirical use of antimicrobials.2 The local antibiogram, Indian Council of Medical Research (ICMR) guidance on rational use of antimicrobials,3 and tenets of good antimicrobial prescription were combined to create a syndrome-wise antimicrobial policy. Multiple specialty-wise meetings were held with all the stakeholders, and their inputs and suggestions were considered before finalizing the document. The document was shared with all the stakeholders and made available on all the hospital desktops for easy future reference. The document has since been updated every two years.To ensure the mindful usage of certain broad-spectrum or high-end antimicrobials, we categorized them into restricted and limited access categories and started monitoring their use. Justification forms were required to be filled for the drugs in the restricted category, while the consumption data alone was tracked for the ones in the limited access category. This enabled us to optimally utilize our human resources towards fewer critical drugs. The justification had to be provided in a decision-making tool within two days of prescription (Figure 1). A system-generated alert to the prescribers and manual oversight by the pharmacy team was also implemented. The antimicrobials were not withheld at any point. These forms were also analyzed to understand the rationale and pattern of using these antimicrobials. Following this, appropriate action of engagement and education was taken where required.
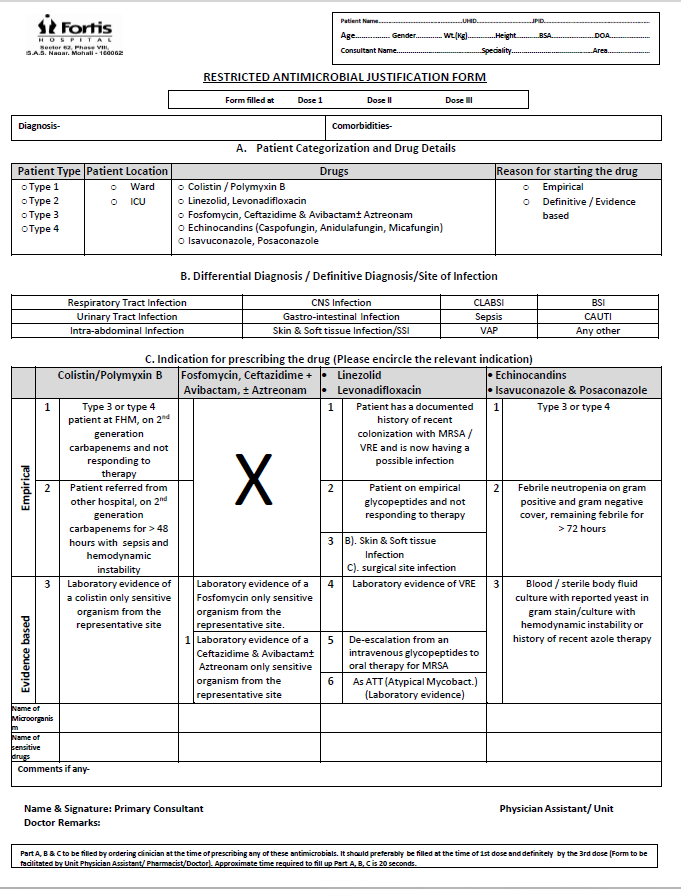

Figure 1: Justification form for restricted antimicrobials
The rationale behind the justification form process was to promote mindfulness over a period of time amongst the prescribers to use these antimicrobials judiciously. Initially, four drugs were categorized as restricted antimicrobials at our hospital (linezolid, polymyxins, fosfomycin, and echinocandins). Lately, ceftazidime-avibactam, aztreonam, levonadifloxacin, isavuconazole, and posaconazole have also been added to this list.
Carbapenems, tigecycline, vancomycin, teicoplanin, daptomycin, and amphotericin B were initially categorized as limited access antimicrobials; minocycline and voriconazole too, have lately been added to this list.
The measurable parameters for the AMS program were identified into process and outcome metrics to look comprehensively at the prescription of antimicrobials.
Process metrics:
The rationale for starting empirical antimicrobials
Appropriate cultures before starting antimicrobials
Inappropriate combination
Therapeutic Duplication
Simultaneous prescription of >= three antimicrobials
Review of antimicrobials once the culture reports are received
De-escalation
Outcome metrics
Total antimicrobial consumption
Defined daily dose (DDD) and days of therapy (DOT)
Drug resistance index (DRI)
Our first Point Prevalence Survey (PPS), in 2107, was based on a tool that included all the above facets of antimicrobial prescription, and we have been participating in all the global PPS surveys conducted since then. These PPS surveys brought forth the low-hanging fruit to be targeted and thus work on those actionables. We also collected and collated the historical annual data on antimicrobial consumption and resistance amongst five key bacterial pathogens and determined the drug resistance index. This served as the baseline data for the outcome parameters we intended to monitor.

Figure 2: Screenshot of the Excel tool used for point prevalence surveys (PPS)
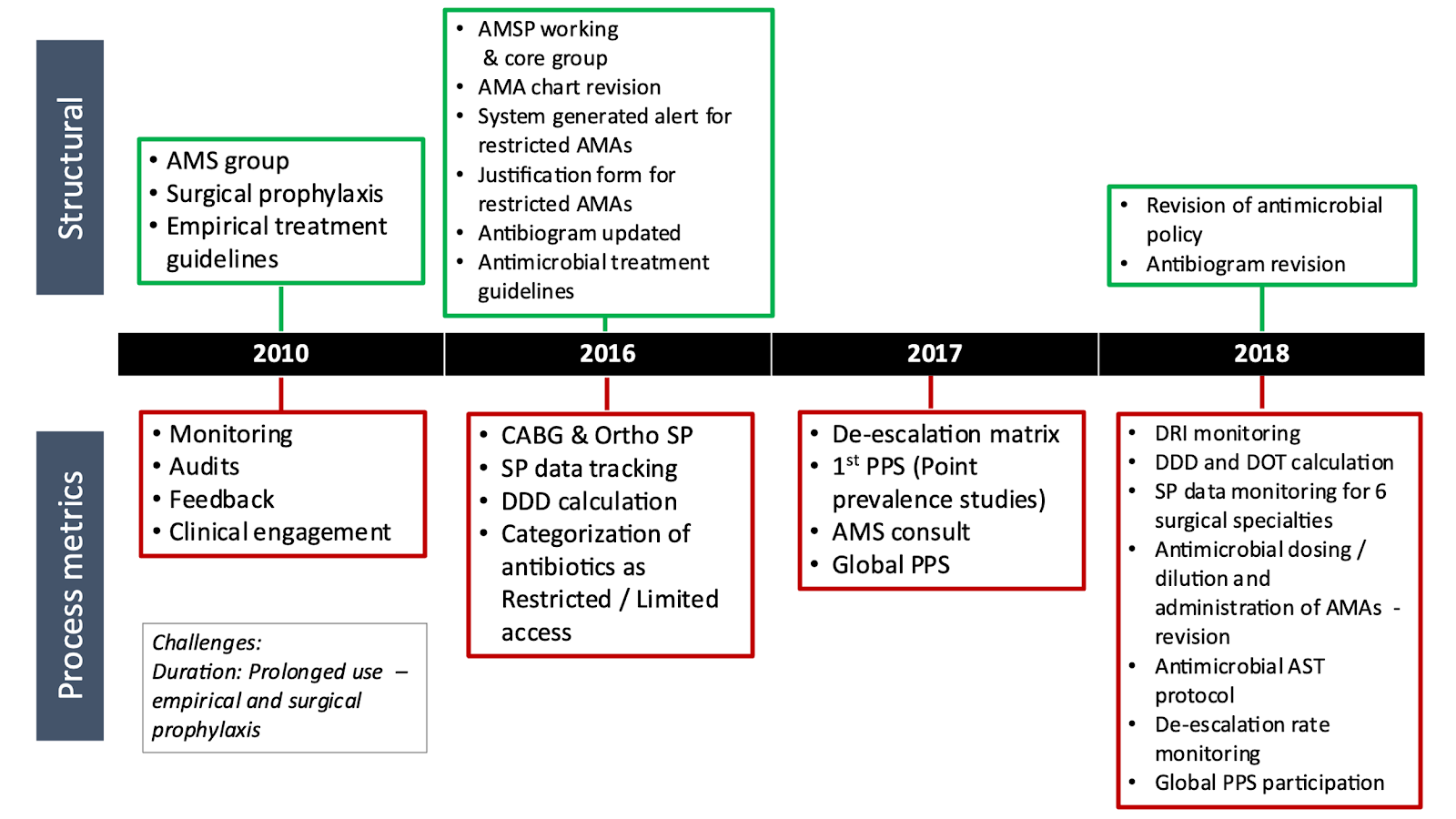

Figure 3: This timeline shows the key elements of our program since its inception
Figure 3 shows the timeline of the key elements of our program since its inception.
CORE ELEMENTS OF OUR PROGRAM
Our organization has put AMS as one of the key performance areas of the leadership, including the Chief Executive Officer (CEO).
The CEO is accountable to the board regarding the outcomes of the program. AMS dashboard (Figure 4) captures the key elements monitored at the board level for every hospital in the network. This ensures a robust governance mechanism at the organization level.

AMS steering committee is the local group responsible for the design and review of the program. It is a multidisciplinary group with representation from clinical and medical administration departments. The recommendations are shared with the Infection control, Quality steering committees, and respective stakeholders. This working group meets monthly, and the proceedings are documented and shared (Figure 5).
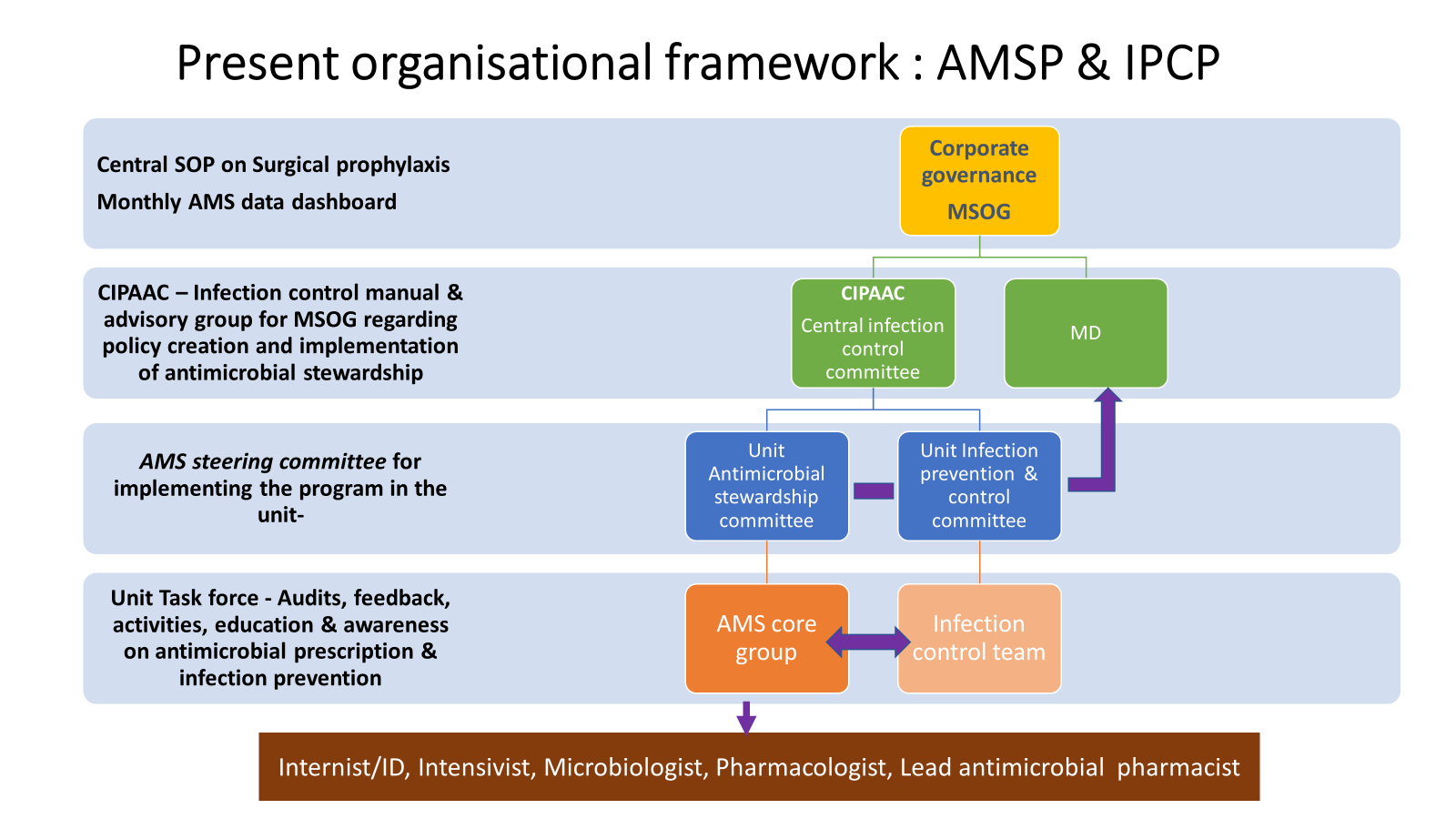
Figure 5: Our organizational framework for the antimicrobial stewardship program and Infection prevention and control program
AMS core group is the functional arm of this committee and consists of a senior intensivist, infectious diseases physician/ internal medicine consultant, microbiologists and infection Control Officer (ICO), clinical pharmacologist, lead antibiotic pharmacist, and an infection control nurse. This core group meets informally on almost a daily basis.
Surveillance audits, Accessibility, Feedback, and Education through engagement (SAFE) are the four cornerstones of our program. This SAFE approach has helped provide a strong foundation for our program and helped it earn respect and credibility within the hospital and outside.
Surveillance audits are undertaken for the following:
Surgical prophylaxis, as recommended in the hospital’s antibiotic policy
Compliance with process and outcome metrics defined for the prescription of empirical therapy.
Compliance with policy recommendations on empirical prescription of antimicrobials (syndromic approach)
Accessibility of members of the AMS core group to all the prescribers 24×7 for any antimicrobial-related query has helped to gain prescriber buy-in regarding the antimicrobial policy recommendations. AMS team provides consultation and support to clinical teams for judicious use of antimicrobials in difficult cases.
Feedback forms the bedrock of our program. We’ve seen that proactive feedback given with the patient’s interest in mind is readily accepted and fosters collegial bonding between the stakeholders, thus enriching the organization’s overall culture. Lead antibiotic pharmacist looks for opportunities for improvement concerning antimicrobials. Any deviations are corrected or escalated to the treating unit and the AMS team for corrective actions. Prospective audit and feedback has been a beneficial strategy for us and will be discussed in depth in the next section.
Education through engagement is an ongoing endeavor at our hospital. Clinical Staff is educated on the rational use of antimicrobials through interactive sessions, classroom teachings, or case discussions. Medical trainees are given particular focus. Antibiotic Awareness Week is celebrated yearly to raise awareness about rational use amongst the medical fraternity and the community. Nurses ensure that the cultures are taken and sent before administering antimicrobials. Training on appropriate techniques for the collection of cultures is periodically undertaken.
GAME CHANGERS IN OUR ANTIMICROBIAL STEWARDSHIP PROGRAMME (AMSP)
These are some of the granular elements that were able to give visible momentum to the program.
Dedicated color-coded antibiotic chart:
When our hospital started, antimicrobials used to be charted along with the other drugs in one combined order sheet. In the absence of electronic medical records (EMR), this would make manual tracking of antimicrobial prescriptions difficult and time-consuming. Separate color-coded (light green) antimicrobial prescription sheets were introduced, and have now been incorporated into every patient’s medical history (Figure 6).
Apart from the essentials related to the prescribed antimicrobial (Name, dose, route, frequency, generic name, starting date), these sheets include
i. Risk stratification of patients based on their previous antibiotic consumption history (Category I/II/III/IV)4
ii. Indications for antimicrobials (Disease condition requiring antimicrobials)
iii. Type of prescription – empirical/ surgical prophylaxis/targeted
iv. Were appropriate cultures sent before the administration of antimicrobials?
v. Review of antimicrobials on days 3, 7 and 10
vi. Antimicrobial susceptibility testing protocol
vii. Antimicrobial dilution protocol
The introduction of these sheets not only enabled more mindful antimicrobial prescriptions but also helped significantly in the antimicrobial audit process.
Lead antimicrobial pharmacist:
Clinical pharmacists have always been a part of our hospital. However, their role and responsibility has been gradually expanding. One of these clinical pharmacists was earmarked as the ‘Lead antimicrobial pharmacist’ and given the additional responsibility of explicitly focusing on antimicrobial usage. Being the senior among all the clinical pharmacists and having an inclination and dedication to self-learning and growth, he has contributed immensely to our program. He is now the custodian of our antimicrobial consumption data and spearheads both the ‘prospective audit and feedback’ and ‘antimicrobial time-out’ processes mentioned below. Many prescribers now directly seek his advice related to drug choice, dosages, and interactions. While focused training on antimicrobials for pharmacists would be an essential step forward, the absence of it should not be a deterrent, as the passion and commitment of pharmacists can more than makeup for it.
Prescriber engagement:
Our program has valued dialogue over demand and engagement over compulsion. From the first baby step of surgical prophylaxis to drafting the hospital’s antimicrobial policy and ensuring that this policy is followed, prescriber and stakeholder engagement has been the way for our program. Concepts of ‘Handshake stewardship’ and ‘IKEA effect’ have added to our conviction that this path,5,6 though more challenging to begin with and surely more time-consuming, eventually leads to longer-lasting and more durable results.

Figure 6: A dedicated antimicrobial administration chart used for every inpatient on antimicrobial(s) at our hospital.
Prospective audit and feedback (PAF): Prospective audit and feedback is the most widely accepted and effective AMS strategy. Though labor-intensive, it relies on ‘immediate concurrent feedback’ and offers rich dividends.7 It has been shown to help decrease the average length of stay, broad-spectrum antimicrobial usage, and antimicrobial cost.8 This intervention has been found useful even in the pediatric setting.9
In 2019-2020, we did a six-month project on Prospective audit and feedback. As part of this project, all inpatients with a positive blood culture report were followed up prospectively by the AMS team (helped by
two clinical pharmacy interns) to see if action was taken upon that positive report. A dialogue with the clinical team was undertaken wherever we found that any action in the form of escalation/de-escalation was
warranted but had yet to be taken by the treating team. This project helped us understand our baseline de-escalation rate and the impact of PAF on improving this rate.
Subsequently, post-COVID, PAF has become a standard of care at our hospital, and our lead antimicrobial pharmacist follows up with all inpatients with positive cultures and initiates dialogue with the treating teams where needed. In situations where he cannot effect a change at his own level, the matter is escalated to senior AMS team members, who then evaluate the situation and initiate a dialogue with the treating team. In every situation, the decision of the treating team remains final, and no change is forced upon the treating team. Their reasons for not agreeing with the AMS team’s recommendations are documented. The following are considered as de-escalations.
Broad-spectrum to narrow-spectrum antimicrobial.
Multiple drugs to a lesser number of drugs
Intravenous to oral
Stoppage of antimicrobials
Antimicrobial time-out (ATO):
This year, in 2023, we have introduced a new concept of ‘antimicrobial time-out’ in our hospital. Unlike PAF, which is more of a ‘third party intervention,’ ATO involves structured mindfulness towards antimicrobial prescription by the prescribers themselves during the routine clinical rounds.10 It is more of a self-stewardship mechanism, like the pre-surgery time-out concept, which has become almost a norm. It has been shown to promote critical thinking on the part of the prescribers.11 Initial hand-holding by the clinical pharmacists by way of pharmacist-led antimicrobial time-out has been reported to be beneficial because of the consistency and knowledge base that they provide to the system.12
We started ATO in one of our ICUs and are taking it to the other ICUs in a phased manner. This, again, is spearheaded by our lead antimicrobial pharmacist. Every patient admitted to the ICU is audited on the day of admission for the correctness of antimicrobial prescription in terms of the choice, dose, route, frequency, and drug-drug interactions. Any change, if warranted, is communicated to the treating team, and the prescription is modified to prevent the error from reaching the patient. Once the cultures are back, the patient is followed up again on day 3 or 4 to see if any change in the antimicrobial prescription is warranted. The same step is repeated on day 7 or 8 and at the time of discharge from the ICU to see if the antimicrobials can be stopped. This multi-step pharmacist-driven antimicrobial time-out has further enhanced the role and acceptance of the lead antimicrobial pharmacist in our hospital and contributed significantly towards our AMS program.
OUR KEY ACHIEVEMENTS
Though the final goals of our program are yet to be achieved, we have indeed been able to earn small but worthwhile wins that have laid a strong foundation for our program. The biggest achievement has been the ‘visibility’ of the AMS team, with many prescribers actively seeking inputs from the core AMS team members in antimicrobial-related queries.
Surgical prophylaxis and de-escalation have been our biggest gains in process metrics. Starting from a situation where SP was often prescribed for almost a week, and broad-spectrum antimicrobials were at times used for this purpose, we are now in a position much closer to the international benchmarks in this context. The concept of de-escalation, too, has seen a similar paradigm shift. Therapeutic duplication has decreased, and inappropriate antimicrobial combinations are used less often. Lately, we have started monitoring our compliance with our antimicrobial policy for a select subset of patients and have found it to be good ( >95%). Though we have seen an improvement in the use of cultures and the appropriate filling up of justification forms, we still need to meet our expectations and benchmarks in these two areas. (Table 1)
Regarding the outcome metrics, we have seen improvement in using restricted and limited access antimicrobials. Our Drug resistance index (DRI) has also improved slightly. Lately, we have started capturing our multidrug resistance organisms (MDRO) rate per 1000 patient days. Improvement in this parameter would be an accurate indicator of the success of our program.
OUR CHALLENGES AND LEARNINGS
Apart from the human behavioral elements that can be a challenge to any program, the key hurdles that we faced in establishing our program have been:
Surgical site infections:
Any infection in a surgical case made the surgical team return to their previous practice and prolong the duration of surgical prophylaxis. This stems out of fear of SSI and its ensuing fallouts like increases in morbidity, mortality, costs of treatment, and medico-legal liability.
High MDRO rate:
Being a tertiary care hospital, we receive critically ill patients who either have a documented MDRO infection or are already on broad-spectrum antimicrobials before coming to us. Choosing a a narrower spectrum empirical antibiotic for them becomes a challenge at times.
Slowly evolving culture of cultures:
Some of our prescribers are yet to imbibe the culture of cultures and are either reluctant to send the
appropriate cultures before starting antimicrobials or find this practice a waste of resources.
Expanding the team of antimicrobial pharmacists:
A solo person can do only so much. Though our lead antimicrobial pharmacist has been a game changer for
us, we find it difficult to add more hands and minds to this cadre.
Infection prevention and control training issues: Non-adherence to infection control (IC) practices due to sudden changes in the staff-patient ratio were the other challenges that often led to setbacks in the program.
Despite these challenges, we have been able to make a significant headway in our program. Critical factors behind this have been multifactorial and multidimensional. Regarding surgical prophylaxis, the first and foremost factor was the commitment of a multidisciplinary core team to conceptualize, collect the evidence, and initiate this program. The presence of good literature was helpful, along with the fact that initiation for surgical prophylaxis was done for clean surgeries where the scope of other confounding variables was minimal. The consensus building amongst various surgical specialties towards writing our SP document ensured an excellent acceptance of the program in principle. Case-to-case addressing of individual concerns helped us overcome implementation challenges wherever they were encountered. Also, identifying a champion (Anaesthetist) was crucial to the success of the surgical prophylaxis vertical, as, in our experience, they are more in a position to make a difference in this aspect. Regular audits and feedback have been our key strategy. Discussing the feedback with the team and listening to their concerns and arguments helped the core team to rework their strategy. Collaboration amongst administration, infection control, engineering, and CSSD provided the collective confidence to stop the antimicrobials early on. Celebrating success with other teams encouraged and motivated others to join the initiative.
Similarly, regarding empirical prescription practices and de-escalation, the critical factor for success has been a multimodal and multidisciplinary approach to resolving the concerns in a participative and engaging manner. Perseverance, celebrating small gains, and returning to the drawing board to re-strategize during failures have ensured that we stay aligned with the program. The active involvement of lead antimicrobial pharmacists has been a crucial factor. Targeting the aspects of antimicrobial prescription by the pharmacist that do not impinge directly on the prescription domain of clinicians, like appropriate dose, route, and double spectrum combinations, ensured easy acceptance of the pharmacist’s involvement in the initial phases. This led to a more incredible rapport and confidence to influence change in behavior and prescription practices as the program matured over the years.
Similarly, the non-binding suggestions the AMS team gave helped build an environment of trust amongst colleagues. Champions were the individuals who sometimes took a leap of faith to try and do things differently than the prevailing environment, especially seen with our surgical prophylaxis vertical. Their commitment and attention to meticulous record keeping ensured robust data availability for use towards change management. The support provided by the administrative control has been of immense help. The governance mechanism has ensured a continuum of accountability for the efforts across the board.
There have also been many setbacks and stalemates that required stepping back often, reenergizing the team, resetting the goals, defining measurables, and engaging peers for group discussions. Increased national and international conversations, guidance documents, and mandate of AMSP by accreditation programs like the National Accreditation Board for Hospitals (NABH) and Joint Commission International (JCI) have strengthened our AMS team to carry on their stewardship activities with renewed vigor.
As we enter the consolidation phase of our program, we intend to amalgamate antifungal stewardship in the ambit of our program. Our ultimate objective is to see AMSP get embedded into the cultural fabric of our organization, with self-stewardship becoming a way of life for all prescribers. We will then be able to celebrate penicillin’s centenary on 28th September 2028 with the gusto it deserves. A journey of a thousand miles begins with a single step, and we have taken some significant steps in this AMSP journey of ours but still have miles to cover.
ACKNOWLEDGEMENT
We would like to acknowledge the immense far-sightedness and contribution of Late Dr. Sonu Malhotra, our Clinical Pharmacologist cum Quality Head, who encouraged us to embark upon this AMSP journey.
CONFLICT OF INTERESTS STATEMENT
The authors declare no conflict of interest.
SOURCE OF FUNDING
None
AUTHORS’ CONTRIBUTIONS
SCV: Conceptualisation, review and editing
AKM: Conceptualisation, writing the draft, review and editing
AS: Writing the draft, review and editing
PKC: Writing the draft, review and editing
SJ: Review and editing
PS: Review and editing
AK: Data curettage and compilation, review and editing
REFERENCES
- 1. Aiken AM, Wanyoro AK, Mwangi J, Juma F, Mugoya IK, Scott JAG. Changing use of surgical antibiotic prophylaxis in Thika Hospital, Kenya: A quality improvement intervention with an interrupted time series design. PLoS One. 2013;8(11):e78942.
2. Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;62(10):e51-e77.
3. Indian Council of Medical Research (ICMR). Treatment Guidelines for Antimicrobial Use in Common Syndromes. Accessed November 25, 2023. http://www.icmr.nic.in/guidelines/treatment guidelines for antimicrobial.pdf
4. Tiwari K, Patil S, Naik A, Shetty A, Walia K, Rodrigues C. Patient risk factor stratification is essential for the hospital antibiogram. Int J Infect Control. 2021;17(1):1-5.
5. Hurst AL, Child J, Pearce K, Palmer C, Todd JK, Parker SK. Handshake stewardship: A highly effective rounding-based antimicrobial optimization service. Pediatr Infect Dis J. 2016;35(10):1104-10.
6. Sikkens JJ, van Agtmael MA, Peters EJG, et al. Behavioral Approach to Appropriate Antimicrobial Prescribing in Hospitals: The Dutch Unique Method for Antimicrobial Stewardship (DUMAS) Participatory Intervention Study. JAMA Intern Med. 2017;177(8):1130-8.
7. Chung GW, Wu JE, Yeo CL, Chan D, Hsu LY. Antimicrobial stewardship: A review of prospective audit and feedback systems and an objective evaluation of outcomes. Virulence. 2013;4(2):151-7.
8. Morrill HJ, Caffrey AR, Gaitanis MM, LaPlante KL. Impact of a prospective audit and feedback antimicrobial stewardship program at a veterans affairs medical center: A six-point assessment. PLoS One. 2016;11(3):e0150795.
9. Chautrakarn S, Anugulruengkitt S, Puthanakit T, Rattananupong T, Hiransuthikul N. Impact of a Prospective Audit and Feedback Antimicrobial Stewardship Program in Pediatric Units in Tertiary Care Teaching Hospital in Thailand. Hosp Pediatr. 2019;9(11):851-8.
10. Thom KA, Tamma PD, Harris AD, et al. Impact of a prescriber-driven antibiotic time-out on antibiotic use in hospitalized patients. Clin Infect Dis. 2019;68(9):1581-4.
11. Graber CJ, Jones MM, Glassman PA, et al. Taking an antibiotic time-out: Utilization and usability of a self-stewardship time-out program for renewal of vancomycin and piperacillin-tazobactam. Hosp Pharm. 2015;50(11):1011-24.
12. Stang CRT, Jaggi P, Tansmore J, et al. Implementation of a pharmacist-led antimicrobial time-out for medical-surgery services in an academic pediatric hospital. J Pediatr Pharmacol Ther. 2021;26(3):284-90.