

KEYWORDS: Antimicrobial utilization; AWaRe; Antimicrobial stewardship
Antimicrobial Stewardship (AMS) refers to the optimal selection, dosing, and duration of antimicrobial treatment resulting in the best clinical outcome with minimal side effects to the patients and minimal impact on subsequent resistance.1,2 World Health Organization (WHO) policy on integrated antimicrobial stewardship activities states that there needs to be evidence-based policies, operational guidelines, standard operating procedures, and implementation tools to facilitate the scale-up of integrated stewardship activities.3 Even though prospective audit-feedback and preauthorization are the commonly used strategies of antimicrobial stewardship, limitations of this strategy include partial compliance, resource intensiveness and long lag period in visible benefits, however it comes with definite reduction in antimicrobial utilization and cost reduction.4 Retrospective audit and feedback is another back end strategy that can be adopted in resource poor setting as an initial step towards implementation of antimicrobial stewardship programme. Patients admitted to the intensive care units (ICU) are seriously ill, while those admitted in the medical ICUs suffer from chronic critical illness, those admitted in the surgical and trauma ICUs have to tide over the morbidity immediately occurring postoperatively or post-trauma.5 The physiological instability and immunocompromised status of the patients admitted to the ICUs necessitate high stakes monitoring to facilitate therapeutic efficacy. Use of broad-spectrum antimicrobials, multiple antimicrobials, and extended length of therapy with antimicrobials can contribute to the growing antimicrobial resistance. ICUs turn out to be the epicenters of antimicrobial pressure accentuated by the altered response of the patients because of organ failure or accentuated renal clearance. Appropriate culture-based escalation, deescalation or step down is necessary for ensuring antimicrobial stewardship. Antimicrobial utilization studies serve as initial steps towards ensuring better antimicrobial stewardship practices. The literature and evidence though present are scanty regarding the pattern of use of antimicrobials in Intensive Care Unit specifically to Kerala. To address this gap this study was devised with an objective to describe the pattern of use of antimicrobials in patients admitted to Intensive Care Units of Government Medical College in Central Kerala.
METHODOLOGY
This was a retrospective study done in the Department of Pharmacology, of a tertiary care centre for a period of one month. Scientific Review Committee and Institutional review board clearance was obtained [IRB 262/2023/GMCK dated 04.07.2023] before initiation of the study. The data collected as a part of the antimicrobial stewardship programme from the Medicine, Surgery and Trauma Intensive Care Units (MICU, SICU, and TICU) of this Government Medical College for a period of one month in 2023 were retrospectively analyzed during Antimicrobial Stewardship electives posting. All the patients who received a single dose of parenteral or oral antimicrobials in the MICU, SICU, and TICU with a stay for at least 24 hours during the study period were included in the study and their data were collected till they were transferred out. Patients who expired in less than 24 hours of admission or use of topical or local antimicrobials were excluded. The antimicrobial name, class of drug, Access Watch and Reserve (AWaRe) classification, incorporation of antimicrobial in the Essential Medicine List, whether the drug was available as single drug or fixed dose combination, the Anatomical and Therapeutic Classification were the different variables.6 The data were analyzed using Jamovi solid version 2.3.28. The Defined Daily Dose was estimated using the World Health Organisation Antimicrobial Consumption Tool.7
RESULTS
This study was done in 11, 18 and 15 bedded ICUs respectively of Medicine, Surgery and Trauma. The total number of patients admitted in Medical ICU (MICU) was eighty-seven of which sixty-two received antimicrobials, those in Surgical ICU(SICU) were 140 of which 119 received antimicrobials and those admitted in Trauma ICU were fifty-one of which forty-six received antimicrobials during the one-month period. A total of 227(81.65%) received antimicrobials amongst 278 patients admitted in the ICUs. Four hundred and seventy-four antimicrobials were prescribed to 227 patients with an average antimicrobial use of 2.09 per encounter.
As shown in Fig 1, the most common antimicrobial prescribed combining all the ICUs was Metronidazole (114,24.05), followed by Piperacillin Tazobactam (65,13.71%) and Cefotaxime (62,13.08%). The most common antimicrobials prescribed in MICU were Piperacillin Tazobactam (24) and Azithromycin (17); SICU were Metronidazole (85) and Cefotaxime (38) and TICU were Metronidazole (26) and Ceftriaxone (24).
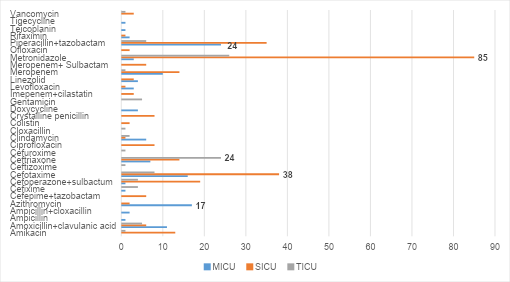
Fig 1: Antimicrobials prescribed in different intensive care units
As summarized in table 1, the most common group of antimicrobials were the bet-lactams 243(51.26%) with 118(24.89%) or without beta lactamase inhibitor 125(26.37%) followed by the Imidazoles 114(24.05%).
Classification of antimicrobials into World Health Organization-Access Watch and Reserve Group is depicted in Figure 2. As shown in the figure2, in all the ICUs majority drugs were from the Watch Category 249(52.53%) followed by the Access category 178(37.55%). The use of Reserve drugs was nine and it was zero in TICU.
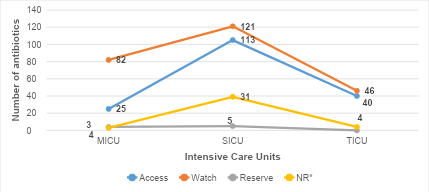
Fig 2: Classification based on WHO-AWaRe 2023 classification.
*NR-not recommended by WHO because of inadequate evidence
Table 2 summarizes the World Health Organisation recommended prescribing indicators. The average antimicrobial use per encounter was 2.09. Of the 474 antimicrobials, 114 were prescribed in the MICU, 270 in the SICU and ninety in the TICU. As shown in Table 3, the antimicrobials prescribed in generic name was 141(29.75%). Majority of the patients received parenteral antimicrobials 432 (91.13%) and 418(88.19%) were from the Essential Drug List. Of the 474 antimicrobials, 346(73%) were single and 128(27%) were fixed dose combinations.
Table 1: Antimicrobial Classification
Table 2: WHO Prescribing Indicators
* Antimicrobials listed in WHO Model List of Essential Medicines 2023
Table 3: Defined Daily Dose
* Ampicillin and Cloxacillin are in Access group, but Ampicillin-Cloxacillin fixed dose combination is placed under Not Recommended list
Figure 3 shows the days of therapy with antimicrobials in the different ICUs. The average days of antimicrobial use in the ICUs was 3.68 ± 3.22 days with a median use of 3(2,5). The average days of therapy was 3.13± 3.03, 3.4± 2.68 and 5.2±4.39 days for MICU, SICU, and TICU, respectively. The length of therapy with antimicrobials ranged from 1 to 21 in MICU with a median of 2 days and IQR (1,4). The length of therapy with antimicrobials in SICU ranged from 1 to 15 with a median use of 3 days and IQR (1.75, 5). In the TICU the length of therapy was from 1 to 24 days with a median use of 4 days and IQR (2,6).
The defined daily dose (DDD) was calculated using the WHO AMC Tool version 1.9. The DDD for each drug is summarized in table 3. The total number of beds in ICU was forty-four and the number of days of study was thirty-one with a 100% bed occupancy, giving a denominator of 1364 bed days. The DDD/100 bed days the ICUs was estimated Anti-infective J was 1677.2 and that for Alimentary A was 8.5. Thirty-one different antimicrobials were used to treat patients for various indications. Eleven were from Access group, seventeen from Watch group and Linezolid as well as Polymyxin from the Reserve group.
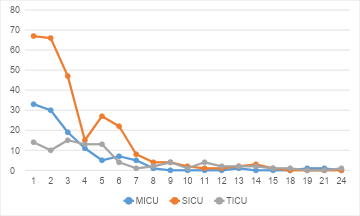
Fig 3: Days of Therapy
DISCUSSION
This study highlights the antimicrobial utilization in different Intensive Care Unit of a tertiary care hospital in Kerala. A qualitative study done in Central Kerala reported challenges in implementation of antimicrobial stewardship with wide use of broad-spectrum antimicrobials hindering stewardship compliance. 8 In the current study 81.65% of the patients admitted in the ICUs received one or more antimicrobials which suggests the importance of strengthening stewardship. Cusack et al. has reported that 71% of the patients in the ICUs could require antimicrobials. 9It could be due to the critically ill situation of patients with multiple organ dysfunction and impaired immunoprotective mechanisms. In 2018, Kerala released Kerala Antimicrobial Resistance Strategic Action Plan (KARSAP) conceptualized and implemented on the One Health platform emphasizing rational prescribing ever since its inception.10 The Smart Antimicrobial Hospital Initiative started in 2024 and revised 2025 in the state of Kerala promotes rational prescribing, prescription audit and reduced Watch group antimicrobial use.11 This study could act as a baseline indicator and benchmark for the further assessments after wider penetration of stewardship practices in the institution in the light of the recent guidelines. In this study, the watch group of antimicrobials accounted for 52.53% of prescriptions with a predominance of ceftriaxone and meropenem.
Syed et al. reported that the ICU patients received beta-lactams (cephalosporins and penicillin) which was in line with this study (51.26% beta-lactams).12In another South Indian study Lavakumar et al., found that cefotaxime/ceftriaxone were the most used antimicrobial agents followed by ampicillin-gentamicin. 5 A study from Nepal by Marsarine et al., has shown that the total antimicrobial utilization in terms of defined daily dose per one hundred bed-days was 49.5 and Piperacillin/tazobactam (45.2%) was the most prescribed antibiotic.13 The current study showed high DDD for the antiinfectives. The WHO surveillance reports indicate that ICU settings worldwide are hotspots for Watch and Reserve antimicrobial use. The analysis performed in 2024 in Southeast Asia has depicted a high consumption of the Watch category pointing towards the need to improve the prescribing in the “Access” category. 14Additionally, the consumption of third and fourth generation cephalosporins was observed to be increasing notably which emphasized tailored interventions for optimizing rational use.14
A study conducted in Malawi found that 52.0% patients received more than one type antimicrobial concurrently ceftriaxone and metronidazole being the most common combination.15 The total average antimicrobial use per encounter in this study was 2.09 with 2.27 in SICU as compared to 2.12 in a study conducted elsewhere.16 The predominance of metronidazole in SICU and TICU is consistent with surgical prophylaxis and anaerobic coverage, however dual and redundant coverage when prescribed with drugs like piperacillin-tazobactam needs to be discouraged. The high parenteral use (91.13%) suggests critically ill patients.16 Evaluation of antimicrobial use in MICU patients found that 73.15% were administered parenterally and there was a mean antimicrobial use of 2.32 per encounter.13 Daily evaluation of signs and symptoms of infection in critically ill patients would ensure adoption of appropriate antimicrobial stewardship strategies.17 Hou et al. and Kitano et al., proposed that antimicrobial consumption decreased by adding stop orders in the antimicrobial stewardship protocols.18,19 Other protocols that could bring about changes with high clinician compliance are the 5 “moments” of antimicrobial prescribing viz, escalation, de-escalation, discontinuation, step down as well as optimization as reported by Devchand et al.20
The strength of this study is that it provides ICU-specific antimicrobial utilization data from Kerala and covers multiple ICUs while integrating prescribing indicators. The short duration, the retrospective design, the lack of microbiological correlation and single centre data are the limitations of this study. There is a need for further documentation of the reasons for antimicrobial use with prospective audits which could bring out more meaningful data.
CONCLUSIONS
This study demonstrates high antimicrobial utilization in Kerala ICUs, dominated by Watch group agents and parenteral therapy, with metronidazole and broad-spectrum beta-lactams, which are most frequently prescribed. The findings suggest the need for robust antimicrobial stewardship programme along with prospective audit-feedback and microbiology-guided prescribing. Strengthening stewardship will help align the WHO recommendations.
CONFLICTS OF INTEREST STATEMENT
The authors declare no conflict of interest
SOURCE OF FUNDING
Nil
AUTHOR’S CONTRIBUTION
KN HS – Protocol Preparation, IRB Clearance, Data collection, manuscript review
AVT – Data cleaning, statistical analysis, manuscript preparation
AE – Data cleaning, data analysis, manuscript preparation
NKV – Data cleaning, data analysis, manuscript preparation
DSP – Idea, Protocol Preparation, IRB Clearance, Data analysis, Statistical analysis, manuscript preparation, corresponding author
HV – IRB clearance, Manuscript review
MOR – Protocol preparation, manuscript review
SK – Idea, manuscript review
SMB – Data analysis, Manuscript review
DECLARATION FOR THE USE OF GENERATIVE ARTIFICIAL INTELLIGENCE (AI) IN SCIENTIFIC WRITING: Declaration for the use of generative Artificial Intelligence (AI) in scientific writing: Nil
REFERENCES
Shrestha J, Zahra F, Cannady J. Antimicrobial Stewardship. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2026 Jan 31]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK572068/
Gerding DN. The search for good antimicrobial stewardship. Jt Comm J Qual Improv. 2001 Aug;27(8):403–4.
World Health Organization. WHO policy guidance on integrated antimicrobial stewardship activities. 1st ed. Geneva: World Health Organization; 2021. 1 p. [cited 2026 Jan 31]. Available online at https://www.who.int/publications-detail-redirect/9789240025530.
Khilnani, G, Zirpe, K, Hadda, V, Mehta, Y, Madan, K, Kulkarni, A, et al. Guidelines for Antibiotic Prescription in Intensive Care Unit. Indian J Crit Care Med. 2019 Jan;23(Suppl 1):S1–63.
Lavakumar S, Arivazhagan N. Drug utilisation pattern of antibiotics in an intensive care unit in a tertiary care teaching hospital in Kancheepuram DT, Tamil Nadu. Int J Cur Res 2017; 9(05):51440-2
World Health Organisation. AWaRe classification of antibiotics for evaluation and monitoring of use, 2023. [cited 2026 January 31]. Available online at https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.04
AMC Tool: The antimicrobial consumption tool. [cited 2026 January 31]. Available online at https://amu-tools.org/amctool/amctool.html [Internet].
Singh S, Menon VP, Mohamed ZU, Kumar VA, Nampoothiri V, Sudhir S, et al. Implementation and Impact of an Antimicrobial Stewardship Program at a Tertiary Care Center in South India. Open Forum Infect Dis. 2019 Apr;6(4):290.
Cusack R, Little E, Martin-Loeches I. Practical lessons on Antimicrobial Therapy for Critically Ill Patients. Antibiotics 2024; 13,162.
Kerala antimicrobial resistance strategic action plan: One Health response to AMR containment: October 2018: Government of Kerala. KERALA ANTIMICROBIAL RESISTANCE STRATEGIC ACTION PLAN (KARSAP). [Last cited 2026 February 1]. Available online at https://cdn.who.int/media/docs/default-source/searo/india/antimicrobial-resistance/karsap-keralaantimicrobialresistancestrategicactionplan.pdf?sfvrsn=ccaa481a_2.
Health and family Welfare Department, Government of Kerala. Standard Operating Procedure for certification process of Antibiotic Smart Hospitals, Antimicrobial Stewardship Compliant Hospitals, Antibiotic Literate Local Self Government and Antimicrobial Stewardship. [Last cited 2026 February 1]. Available online at https://eoffice.kerala.gov.in/EofficePortal/searchIssueStatusBlock2.action.
Syed MHN, Kumar CU, Shobha JC. Prescription Patterns of Antibiotics in Acute Medical Care Unit of a Tertiary Care Hospital in India. 2014;3(7):673-9.
Marasine NR, Shrestha S, Sankhi S, Paudel N, Gautam A, Poudel A. Antibiotic utilization, sensitivity, and cost in the medical intensive care unit of a tertiary care teaching hospital in Nepal. SAGE Open Med. 2021 Sep 3;9:20503121211043710.
World Health Organization. Consumption and rational use of antimicrobials in South-East Asia region. New Delhi: Regional Office for South-East Asia; 2024.
Kayambankadzanja RK, Lihaka M, Barratt-Due A, Kachingwe M, Kumwenda W, Lester R, Bilima S, Eriksen J, Baker T. The use of antibiotics in the intensive care unit of a tertiary hospital in Malawi. BMC Infect Dis. 2020 Oct 19;20(1):776.
Chavhan GK, Abraham JP, Upadhyaya SA, Bokare SP. Antimicrobial usage in post operative patients in general surgery wards and intensive care units of a tertiary care hospital in central India: an ATC/DDD-based observational study. International Journal of Basic & Clinical Pharmacology. 2025 ;14(4):544–9.
Campion M, Scully G. Antibiotic Use in the Intensive Care Unit: Optimization and De-Escalation. J Intensive Care Med. 2018 Dec;33(12):647–55.
Hou D, Wang Q, Jiang C, Tian C, Li H, Ji B. Evaluation of the short-term effects of antimicrobial stewardship in the intensive care unit at a tertiary hospital in China. PLoS ONE 2014;9(7):e101447
Kitano T, Takagi K, Arai I, Yasuhara H, Ebisu R, Ohgitani A, et al. A simple and feasible antimicrobial stewardship program in a neonatal intensive care unit of a Japanese community hospital. J Infect Chemother 2019;25(11):860–5.
Devchand M, Stewardson AJ, Urbancic KF, Khumra S, Mahony AA, Walker S, et al. Outcomes of an electronic medical record (EMR)-driven intensive care unit (ICU)-antimicrobial stewardship (AMS) ward round: assessing the “Five Moments of Antimicrobial Prescribing. Infect Control Hosp Epidemiol 2019;40(10):1170–5.